

Hair transplant necrosis is the death of scalp tissue, skin, grafts, or both, when the blood supply to the treated area is interrupted long enough for cells to die. It is the most serious complication of hair restoration and also one of the rarest.
In Vera Clinic Academy’s Complication and Side-Effect Incidence Registry of 690 patients treated between January 2023 and December 2024, no cases of ischemic scalp necrosis were recorded. Necrosis is driven by identifiable factors: excessive epinephrine, overly dense graft packing, oversized punches, heavy smoking, and untreated infection. Its warning signs, disproportionate pain, dusky or blackening skin, blistering, and non-healing tissue, differ clearly from normal crusting or shedding. Recognising these signs early, knowing which patients carry higher risk, and choosing a clinic with controlled anesthesia and calculated spacing protocols are what keep this complication close to zero.
Key Points
- Hair transplant necrosis is the death of scalp tissue when blood supply to the treated area is cut off; it is the most severe but least common complication of hair restoration.
- Vera Clinic Academy recorded 0 cases of ischemic scalp necrosis across 690 patients treated between January 2023 and December 2024.
- The main causes are controllable: excessive epinephrine, overly dense graft packing, punches wider than 0.9 mm, heavy smoking, and untreated infection.
- Warning signs include disproportionate pain, dusky or blackening skin, blistering, foul odour, and non-healing tissue, all of which need same-day clinical review.
- The highest-risk patients are heavy smokers, those with poorly controlled diabetes, and those with prior scalp scarring or radiation.
- Vera Clinic keeps the risk near zero with controlled-epinephrine tumescent fluid, sub-0.9 mm micro-punches, and calculated recipient-slit spacing.
What Is Hair Transplant Necrosis?
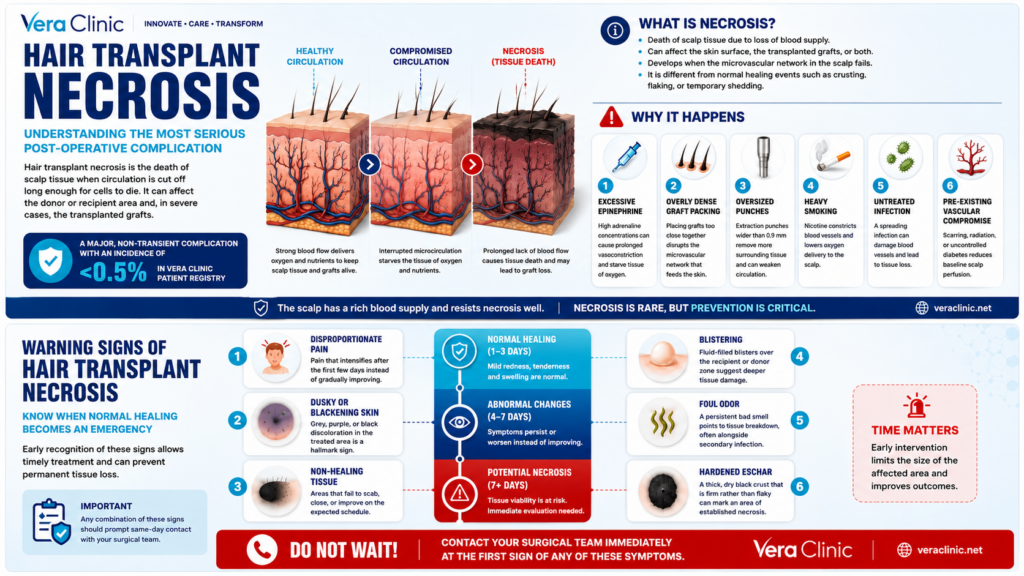
Hair transplant necrosis is the death of scalp tissue when circulation to the donor or recipient area is cut off long enough for cells to die. It is the most severe complication in hair restoration and sits apart from routine healing events such as crusting, flaking, or temporary shedding. Necrosis can affect the skin surface, the transplanted grafts, or both, and it develops when the microvascular network in the scalp fails rather than as a stage of normal recovery.
Vera Clinic Academy classifies necrosis among major, non-transient complications, a category with an overall incidence below 0.5% in its patient registry. Because the scalp carries a dense blood supply, healthy tissue resists necrosis well, and the complication is tied to specific surgical and patient factors rather than to hair transplantation itself. Placing necrosis within the wider set of side effects of hair transplant helps separate a genuine emergency from expected post-operative change.
How Common Is Necrosis After a Hair Transplant?
Necrosis after a hair transplant is rare. In Vera Clinic Academy’s Complication and Side-Effect Incidence Registry, no cases of ischemic scalp necrosis were recorded across 690 patients treated between January 2023 and December 2024, with follow-up continuing through December 2025. The cohort was drawn from 780 consecutive patients, of whom 90 were excluded for incomplete records or loss to follow-up, leaving 690 analysed. Procedures were split between Sapphire-tip FUE (62.0%) and DHI with implanter pens (38.0%), each with a minimum 12-month follow-up.
| Complication | Incidence in the Vera Clinic Academy registry | Notes |
|---|---|---|
| Ischemic scalp necrosis | 0 of 690 patients | No cases observed over the study period |
| Macroscopic or keloid scarring | Below 0.15% of cases | Isolated cases at the 12-month milestone |
| Acute bacterial scalp infection | 0.29% of cases | Resolved within 7 days on oral antibiotics |
| Major non-transient complications (all) | Below 0.5% of cases | Combined category |
These figures place necrosis at the extreme low end of the risk spectrum, far below more familiar concerns such as temporary shedding or scalp itching.
Complication and Side-Effect Incidence RegistryWhat Causes Necrosis After a Hair Transplant?
Necrosis develops when blood flow to the scalp is compromised during or after surgery. The main drivers are technical and patient-related factors, most of which are controllable.
- Excessive epinephrine: High adrenaline concentrations in the anesthetic solution can cause prolonged vasoconstriction that starves tissue of oxygen.
- Overly dense graft packing: Placing grafts too close together disrupts the microvascular network that feeds the recipient skin.
- Oversized punches: Extraction punches wider than 0.9 mm remove more surrounding tissue and can weaken donor-area circulation.
- Heavy smoking: Nicotine constricts blood vessels and lowers oxygen delivery, raising the risk of tissue death in both the donor and recipient zones.
- Untreated infection: A spreading bacterial infection can damage local blood vessels and progress to tissue loss if it is not managed early.
- Pre-existing vascular compromise: Scarring, prior radiation, or poorly controlled diabetes reduces baseline scalp perfusion before surgery even begins.
The recurring mechanism across these causes is interrupted microcirculation, which is why prevention centres on protecting scalp blood flow. Clinical literature identifies excess epinephrine and overly dense packing as the two most frequent triggers (Kerure and Patwardhan, 2018).
What Are the Warning Signs of Scalp Necrosis?
Scalp necrosis produces signals that differ from normal healing and call for same-day clinical review. Early recognition allows treatment before tissue loss becomes permanent.
- Disproportionate pain: Pain that intensifies after the first few days, rather than fading, can indicate failing circulation.
- Dusky or blackening skin: Grey, purple, or black discoloration in the treated area is a hallmark sign of dying tissue.
- Blistering: Fluid-filled blisters over the recipient or donor zone suggest deeper tissue damage.
- Foul odour: A persistent bad smell points to tissue breakdown, often alongside secondary infection.
- Non-healing tissue: Areas that fail to scab, close, or improve on the expected schedule signal compromised viability.
- Hardened eschar: A thick, dry black crust that is firm rather than flaky can mark an area of established necrosis.
Any combination of these signs should prompt immediate contact with the surgical team, because early intervention limits the size of the affected area.
How Can You Tell Necrosis Apart From Normal Healing, Shock Loss, and Infection?
Most post-transplant changes that alarm patients are normal healing events, not necrosis. A recurring concern at Vera Clinic is patients mistaking normal flaking or breakthrough pimples for tissue death; the registry shows these affect 41.2% and 22.7% of patients respectively and resolve on their own.
| Condition | Appearance | Timing | Pain | Resolution |
|---|---|---|---|---|
| Normal crusting and flaking | Dry scabs and dandruff-like flaking around grafts | Itching days 5 to 14; flaking weeks 2 to 6 | Mild itching in 68.4% of patients | Self-resolving |
| Shock loss | Sudden shedding of existing or transplanted hairs | Weeks 2 to 8 | None | Regrows within months |
| Infection | Pustules, redness, tenderness, discharge | First 1 to 2 weeks | Localised soreness | Clears on antibiotics; 0.29% of cases, within 7 days |
| Necrosis | Dusky, blackening, non-healing skin | From the first days, progressive | Disproportionate and worsening | Requires clinical treatment |
Temporary shedding, known as shock loss after hair transplant, resolves on its own as follicles re-enter the growth phase. Pustular inflammation points to a hair transplant infection rather than necrosis and clears with prompt antibiotic treatment in the small share of patients affected.
Who Is at Higher Risk of Necrosis?
Some patients carry a higher baseline risk because their scalp circulation or healing capacity is reduced. Vera Clinic screens for these factors before approving surgery.
- Heavy smokers: Nicotine-driven vasoconstriction lowers scalp oxygenation, and Vera Clinic requires stopping smoking before and after surgery or defers the procedure.
- Poorly controlled diabetes: Impaired microcirculation and slower healing raise the risk, so blood sugar control is confirmed before scheduling.
- Prior scalp scarring or radiation: Fibrotic or irradiated skin has fewer functional vessels, so dense placement in these areas is avoided.
- Very high-density requests: Patients asking for graft densities beyond what the scalp can safely perfuse are counselled toward safer targets.
- Complex revision cases: Repeat surgery on previously operated scalp carries reduced vascular reserve and is planned conservatively.
Where these risks are significant, Vera Clinic reduces planned density, stages the procedure across sessions, or declines surgery rather than accept a raised risk of tissue loss. The clinic’s position is that a safe, viable result outweighs meeting a density target that the scalp cannot support.
How Does Vera Clinic Prevent Necrosis?
Vera Clinic’s prevention protocol targets the two leading causes of necrosis, compromised blood flow and disrupted microcirculation, through standardised anesthesia and placement parameters.
- Controlled-epinephrine tumescent fluid: The anesthetic solution combines saline, lidocaine, and low-concentration epinephrine to achieve stable vasoconstriction without cutting off dermal blood supply.
- Sub-0.9 mm micro-punch harvesting: Donor extraction uses motorized punches held between 0.7 mm and 0.9 mm to limit tissue removal and protect donor-area circulation.
- Calculated recipient-slit spacing: Recipient sites are opened at structurally safe distances so grafts receive adequate blood flow instead of being packed to the point of vascular strain.
- Strict perioperative sterility: Sterile protocols held the bacterial infection rate to 0.29% in the registry, preventing infection-driven tissue damage.
- Patient aftercare compliance: Gentle handling and avoiding smoking in the early weeks protect the new blood-vessel network as it forms.
This combination is the reason no necrosis cases appeared across 690 patients in the Vera Clinic Academy registry, and it reflects the clinic’s view that safe spacing matters more than maximum density. Following a structured hair transplant aftercare routine in the first weeks supports the same blood supply the surgical protocol is built to protect.
How Is Necrosis Treated If It Occurs?
If necrosis develops, treatment focuses on removing dead tissue, controlling infection, and preserving as much healthy scalp as possible. Early management limits the final size of the affected area.
- Prompt assessment: The surgical team evaluates the extent and depth of tissue damage as soon as signs appear.
- Conservative wound care: Small areas are managed with dressings and monitoring to support natural healing at the margins.
- Debridement: Non-viable tissue is removed to stop progression and allow healthy tissue to close the wound.
- Targeted antibiotics: Antibiotics are added when infection accompanies the necrotic area.
- Eschar management: A stable black crust is monitored or removed depending on the condition of the tissue beneath it.
- Secondary reconstruction: Once the site heals, scar revision or a further graft session can restore coverage in the affected zone.
Grafts within a necrotic area do not survive, so any regrowth there depends on a later revision once the tissue has fully recovered.
Why Choose Vera Clinic for Safe Hair Transplantation?
Vera Clinic pairs European standards with an audited safety record that few clinics can document. The Vera Clinic Academy Complication and Side-Effect Incidence Registry tracked 690 patients through a full year of follow-up and recorded zero cases of scalp necrosis, alongside a major complication rate below 0.5%. This outcome reflects deliberate choices: needle-free high-pressure anesthesia that reduced infiltration pain by 63.79%, controlled tumescent solutions, sub-0.9 mm micro-punches, and recipient-site spacing designed to protect blood flow. Patients choosing Vera Clinic receive a protocol built on measured results and transparent institutional data, with continuous quality auditing through Vera Clinic Academy.
Frequently Asked Questions
Necrosis signs appear early, within the first several days to two weeks after surgery. Warning signals such as worsening pain and darkening skin show earlier than normal healing milestones, which is why any change in the first week should be reviewed by the surgical team.
Necrosis itself cannot be reversed, because the affected tissue has already died. Early treatment can stop it from spreading and preserve the surrounding healthy skin, and once the area heals, scar revision or a further graft session can improve appearance and coverage.
Necrosis can leave a permanent bald or scarred patch where tissue and grafts were lost, since dead follicles do not regrow. The size of the patch depends on how early the necrosis was caught and treated, and a later revision procedure can often restore coverage.
A second hair transplant can restore an area affected by necrosis once the scalp has fully healed and the scar tissue has stabilised. The surgeon assesses blood supply in the scarred zone first, because compromised circulation influences how many grafts the area can safely support.